

Shoulder impingement, dinosaurs, the moon landing, and other made up things
and how to deal with shoulder pain

My favorite way to fix shoulder impingement?
I pretend it doesn’t exist. Magically cured.
Technically this is true since the shoulder “impinges” every time you move it. The diagnosis was created BEFORE we understood how the shoulder worked.

This is a long “education” post, so if you just want to fix your shoulder now just start here

Keep going and I’ll discuss the types of impingement, how to manage it, and what to expect for healing.
Do I have impingement?
Common complaints
Reaching over head, in front, or across your body
Throwing motions, reaching behind you, or putting on a shirt/jacket
Pain on the front of the shoulder or radiates down the arm
Unable to sleep on the that side
Impingement tests to diagnosis it
To diagnose shoulder impingement, you tell me where it hurts, I do a “test” that mimics that motion, and you confirm that that movement hurts, therefore the test is “positive.”
Shoulder impingement only highlights that pain is present, not what in the shoulder actually hurts. Knowing the 2 types of impingement helps.
External (primary and secondary)
Internal

External Impingement
We actually don’t say impingement anymore, we say Subacromial Pain Syndrome.
Shoulder “impingement” ALWAYS occurs, even in pain free shoulders. That red spot is the subacromial space.

The acromion or coracoacromial ligament is compressing a structure (bursa/tendon) under (sub) the acromion. You feel pain because that irritated structure gets smooshed, similar to how a bruise works.
There are 2 types of EXTERNAL Shoulder Impingement
Primary External Impingement
Primary means a structural cause. A common thing to blame is acromion type. You can see in the not realistic cartoon sketch below there are 3 types. Notice Type III has a scary looking hook making the space more narrow, making it easier to compress the tissues.
It looks scary too since it’s basically a hook straight out of a horror movie slashing your rotator cuff. Rest assured that is NOT happening.

The issue of acromion type is debated for a few reason.
One, there’s no good way to measure it.
Two, cuff tear severity is not related to acromion type. There’s big tears with Type 1, and small tears with Type III.
Third and final, you don’t have a choice since it’s possible your type is predetermined. They did a study where they looked at a bunch of shoulders and saw a variety of types, so they thought it changed over time.
Then they did a study where they looked at a bunch of the same shoulders over 3 years and none of them changed. It’s possible 3 years isn’t long enough.
Basically we don’t know shit.
It’s likely all related to overall rotator cuff muscle quality. So, you know, you should exercise.
Secondary External Impingement
Secondary is related to impaired strength and mechanics of the cuff muscles and the scapula muscles. So, you know, you should exercise.
Both primary and secondary shoulder impingement likely have strength and ROM deficits, secondary won’t have (as much?) associated structural stuff. Makes sense since…
Primary is the most common and usually affects older (> 40yo) folks.
The longer you are alive, the greater chance to get all these things. Another argument for tissue quality. So, you know, you should exercise.

Internal Impingement
This is pain in the back of the shoulder and common in baseball pitchers. It is an adaptation to throwing since pitching is a violent motion for the shoulder.
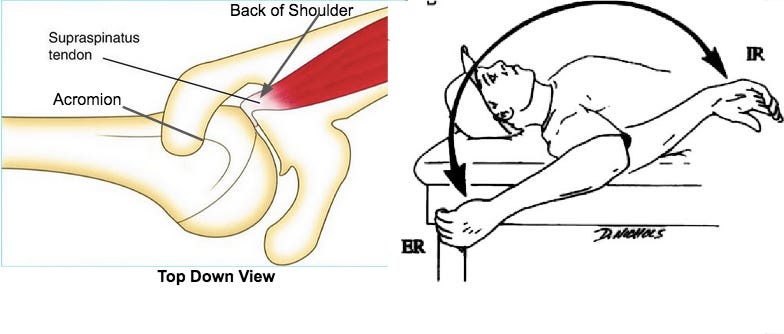
You may also have reduce ROM overhead and the front of your shoulder can be “loose” to allow that much extra ER ROM. This can later lead to a cuff tear or labrum issues.
Pain is felt in the back of the shoulder (left picture) in the late cocking phase of throwing or putting on a jacket.

I’ve currently treating a 17 yo female in the band and a 43 yo male fighter pilot that have ROM just like the baseball player picture above. The female’s symptoms are NOT consistent with internal impingement, the pilot’s are.
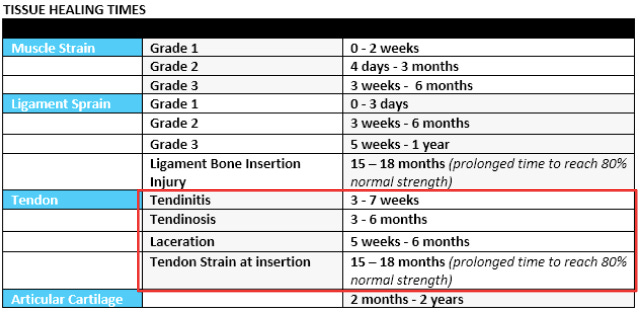
What to expect with healing
Tendons don’t have as good of a blood supply as muscles, so it can take longer to heal.

Depending on the severity, you have to think in terms of months, not weeks.
Pain is not a good indicator of what’s going on in the tendons (or muscles). You can have no pain but the tendon has low tolerance, so as soon as you start pushing the intensity (heavier weight, faster speed, etc), the pain can come back if you exceed your tolerance.
As long as pain is kept within tolerance, you can keep progressing. Aim to keep pain less than 4/10 with activity.
How to Fix Shoulder Impingement
Treatments for each all involve the same thing – treat the impairments.
range of motion
strength deficits/tissue quality
slowly progress back to activities
I already linked a great shoulder rehab program at the beginning of the article, start there if the pain is new.
Paid subs get that PLUS our Shoulder Rehab 1.0

upgrade here >>> become a paid sub